A classifier to predict viral control after antiretroviral treatment interruption in chronic HIV-1 infected patients
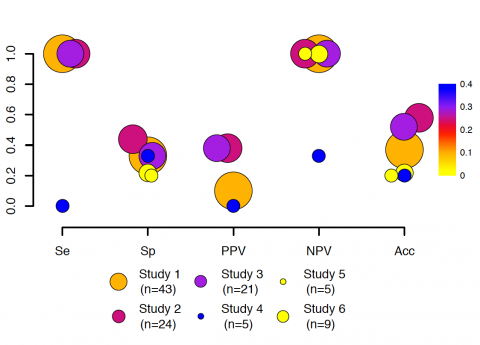
Feher C, Plana M, Guardo AC, Climent N, Leal L, Ugarte A, fernandez I, Florencia Etcheverry M, María Gatell J, Sanchez-Palomino S, GarcÍa F, Aloy P, OBJECTIVES: To construct a classifier that predicts the probability of viral control after analytical antiretroviral treatment interruptions (ATI) in HIV research trials. Participants of a dendritic cell-based therapeutic vaccine trial (DCV2) constituted the derivation cohort. One of the primary end-points of DCV2 was the drop of viral load (VL) set point after 12 weeks of ATI (delta VL12). We classified cases as "controllers" (delta VL12 >1 log10 copies/mL, n=12) or"non-controllers" (delta VL12 < 0.5 log10 copies/mL, n= 10), and compared 190 variables (clinical data, lymphocyte subsets, inflammatory markers, viral reservoir, ELISPOT, and lymphoproliferative responses) between the two groups. Naïve Bayes classifiers were built from combinations of significant variables. The best model was subsequently validated on an independent cohort. Controllers had significantly higher pre-ART VL (110250 [IQR 71968- 275750] vs. 28600 [IQR 18737-39365] copies/mL, p=0.003) and significantly lower proportion of some T lymphocyte subsets than non-controllers: pre-vaccination CD4+CD45RA+RO+ (1.72% vs. 7.47%, p=0.036), CD8+CD45RA+RO+ (7.92% vs. 15.69%, p=0.017), CD4+CCR5+ (4.25% vs. 7.40%, p=0.011), and CD8+CCR5+ (14.53% vs. 27.30%, p=0.043), and post-vaccination CD4+CXCR4+ (12.44% vs. 22.80%, p=0.021). The classifier based on pre-ART VL and pre-vaccine CD8+CD45RA+RO+ T cells was the best predictive model (overall accuracy: 91%). In an independent validation cohort of 107 ATI episodes, the model correctly identified non-responders (negative predictive value=94%), while it failed to identify responders (positive predictive value=20%). Our simple classifier could correctly classify those patients with low probability of control of VL after ATI. These data could be helpful for HIV research trial design.
Journal of Acquire Immune Deficiency Syndrome,
2020
METHODS:
RESULTS:
CONCLUSIONS:
Pubmed: 31904703
Direct link: 10.1097/QAI.0000000000002281